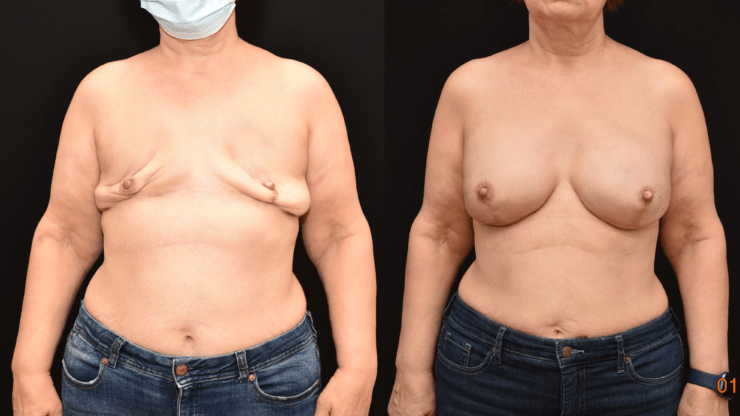
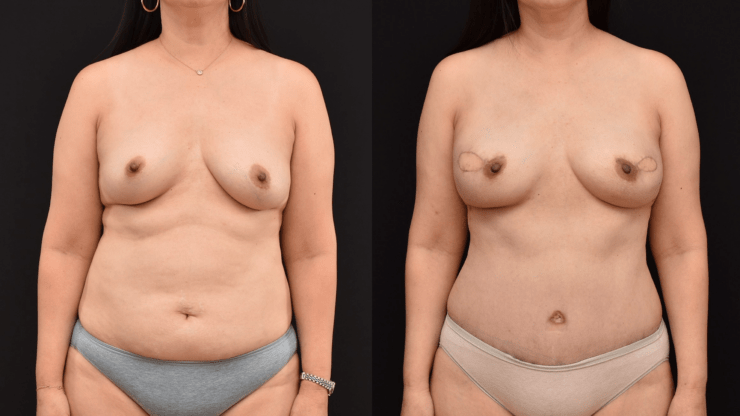
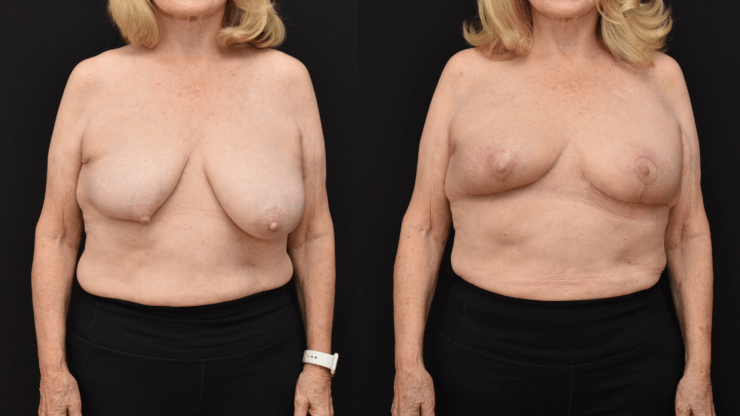
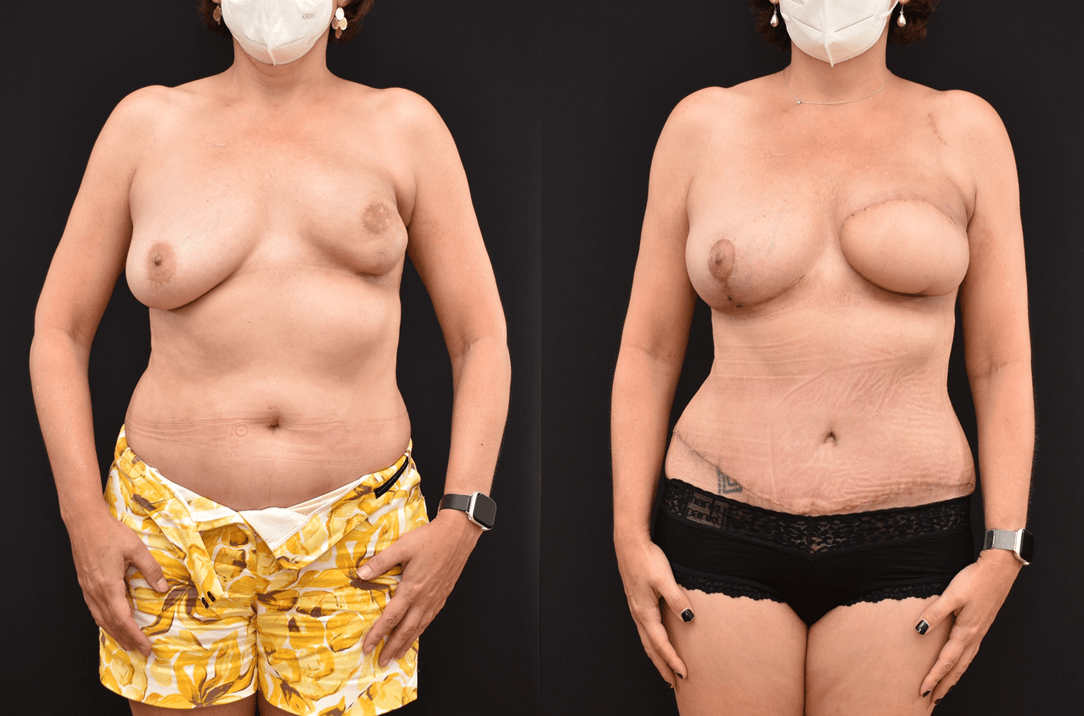
Breast reconstruction is a challenging specialty in plastic and reconstructive surgery. Not only does the patient and reconstructive surgeon have to contend with a foreign object of the mammary prosthesis, but also chemotherapy and radiation which can make the reconstructive process more challenging. The photograph demonstrates before and after implant reconstruction of bilateral mastectomy defects with bilateral mammary prosthesis. The…